
Who, what & why?
It’s a question we get asked a lot at ithlete: should I take my morning measurement lying down in bed, or standing up? Our response has always been that if you have a low resting heart rate (less than 55 bpm), then you should be doing the reading standing up. This is to avoid an effect called parasympathetic saturation, which occurs when you get very fit: your heart and blood vessels become very efficient, so the brakes to your heart rate are fully on when you are lying down at rest. In theory, this makes daily HRV readings less sensitive to changes in training loads and lifestyle stress.
Although this has been known for a few years, recently, researchers in the Czech Republic decided to put it to the test in a detailed study on an elite fin swimmer during their 6 month training period before the World Championships.
What did they do?
The researchers monitored an elite female fin swimmer during 3 phases of training over the 6 months, and the period including travel to a distant location (Colombia) where she performed her final preparations for the games. HRV readings were taken in the lying down (supine) and standing positions, using medical grade ECG equipment every training day in the morning after waking. Neither the athlete, nor the coach knew the results and continued to adjust her training using traditional training load & subjective (fatigue) measures.
What did they find?
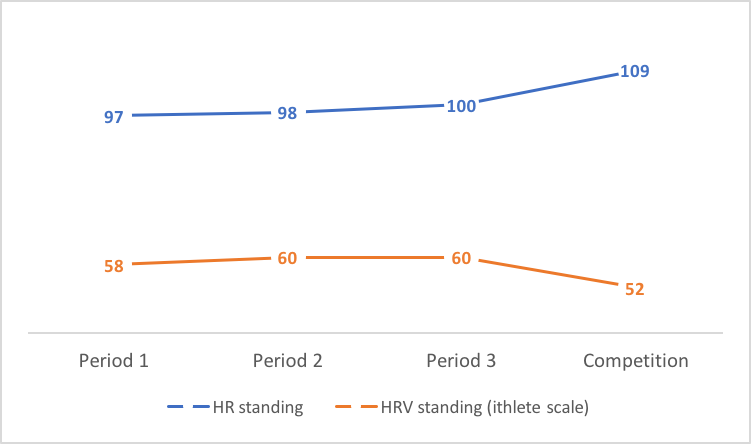
They found no significant changes in HRV or resting heart rate during the Period 1 & 2 build phases, nor during the pre-competition taper Period 3, where volume was reduced to 50% of the previous period, but intensity maintained. The interesting findings were during the monitoring at the competition location, which involved lengthy travel, 6 time zones away from the athlete’s home. This chart shows that the supine HRV and HR remained essentially unchanged throughout:
whereas the HRV readings taken in the standing position dropped significantly, and the resting HR increased significantly:
What does it mean?
Regarding the lack of change during the training build phases, the authors concluded that ‘the athlete is so well-trained (adapted) that the changes in the amount of load do not induce a significant stress response leading to changes in autonomic cardiac regulation in the supine position’ but that ‘It is apparent that the accumulation of stress factors in the form of training, competition stress, and flying over time zones induces a significant response of the regulatory system, but detectable only in the standing position.’ They also made the interesting observation that the lowered HRV and raised resting HR immediately prior to competition did not hurt the athletes performance – in fact she delivered a personal best at the games. This is quite commonly observed by ithlete users as a race day amber or red – if your HRV has been good during taper and you have not become sick, then this is not going to hurt your performance, and in fact could be a helpful stress response preparing you for the ‘fight or flight’ that awaits.
In another recent study on recreational runners, researchers at KIHU in Finland found that nocturnal HRV was more sensitive to the previous day’s training than measures the next morning, either supine or standing. This could be explained because the nighttime measures were taken during the first 4 hrs of (deep) sleep, when the body is in repair mode; testosterone and human growth hormone are most active, and it does not necessarily reflect the state of recovery the body has reached the next morning.
In summary, HRV readings taken standing up do appear to be more sensitive to accumulated stress, especially in well trained athletes, and this confirms our recommendation for anyone with a resting HR lower than 55 bpm. It’s likely that seated position represents a good halfway house for those with resting heart rates between 50 and 65 bpm, but further research is needed to confirm this.
By: Simon Wegerif
ZUZANA SVOZILOVÁ, MICHAL BOTEK, ZBYNĚK SVOZIL, JAKUB KREJČÍ
Faculty of Physical Culture, Palacky University Olomouc, Olomouc, CZECH REPUBLIC
Published online: Octomber 31, 2017
DOI:10.7752/jpes.2017.s4219
If you have a higher resting HR Thank 55 is it then wrong to do a standing measurement?
Hi Christian. Not a problem to do all your measurements standing even if your resting HR is higher than 55 bpm.
I’ve been measuring HRV laying down, but my HR averages around 48 bpm. If I switch to seated measurements, how long should I count on this change to be averaged out?
Hi Yomina. If you switch to seated, you can expect the baseline to have adjusted within a week or so to the lower level. During this time you might get more amber / red warnings than usual, but these will return to normal.
Hi Simon, I’ve been trying HRV monitoring for 3 months and with no success – very frustrating.
Just heard you on a podcast – and you say (as you do here) that if your resting is below 55, then should to HRV measure whilst standing. Excellent to hear this :-)
BUT – I may have an ectopic heart beat …… well, I have gaps in my heart rate recordings. I started to record my heart beats when the HRV measurements were giving me out of band results.
In your experience – could the gaps in my heart rate recordings be purely this symptom ? that is, because I am so fit, and have a resting heart rate of about 42-44, that the heart rate recordings wont be a true reflection as the body is so calm ?
Any advice regarding ectopic heart beats and false ectopic heart beats from super low heart rates etc. would be greatly appreciated.
Thanks so much
Michael Rensforfd
Sydney, Australia
Hi Michael.
Thanks for the message – your raise a couple of interesting points:
1) What happens when trying to take HRV measures if you have a very low resting heart rate is called ‘parasympathetic saturation’. When you are lying down, this means that the ‘brakes’ to the heart are fully on, and you see very little change in HRV from one day to the next. So, yes, you should be doing the HRV tests consistently in the standing position, where the brakes come off – your HR will be higher standing.
2) Any kind of arrhythmia (ectopic beats, atrial fibrillation) will corrupt the HRV calculations, making the number unrealistic (and often wildly high!). Most apps do have some artifact detection, but if you have several ectopic / AF beats during the measure, it is almost certain to be corrupted. ithlete stops the measure if it finds more than 5 in a minute.
Many masters athletes do have occasional arrhythmia and its not necessarily anything to worry about, but you should get it properly checked out to be sure. If you only get this occasionally, hopefully you can find a clear minute to do your ithlete reading.
Hope this helps, thanks again for getting in touch!
Simon
Hi Simon. Would you believe …. i only just discovered you reply today – in September. Thank you so much for your reply, it is most helpful and validates my conclusions back in January. I did get a 24hr test, some mild ectopic beats going on – some skipped beats in the dead of night (which is interesting – no best for 3 secs) – so I’m no longer pursuing HRV measurements but rather keeping an eye on my sleep resting heart rate and my day time resting heart rate to gauge just how well rested I am. As a means of validating actually how I feel and how I’m performing.
Ultimately the big giveaway is a sky high heart rate when I first start running – way way above threshold heart rate when I’m only warming up tells me straight away that I’m not adequately recovered for the run I’m about to do, so I just take it easy and focus on more food and more sleep the next 2-3 days before trying a harder training session.
Thanks again, Michael R
Hi Simon, I would like to ask about correct procedure for standing measurements. How long should I wait between standing up and starting measurement? I usually wait under 1 minute but then during the measurement I see HR changes a lot in first 5-10s. Not sure if it’s a problem for ithlete algorithm or should I wait standing longer for like 2 or 3 minutes?
Hi Tomas. Thanks for the question. ithlete checks that your heart rate is in the range of ±3 bpm before it will allow the measurement to start and the button turns green. But if you are concerned, there is no problem in waiting for an additional 1-2 minutes before pressing start.
I would be interested to hear if the daily variation in your readings decreases after you do this for a few weeks.
best regards,
Simon.
I have been wondering why my HRV while laying down sleeping overnight is consistently low at 35-38 with minimal variation but at soon as I take my HRV measurement in the morning when I stand up it is significantly higher, ranging anywhere from high 60s to 90s. My resting heart rate is low 50s. Should I not be worried about my low readings overnight and just be focusing on my standing morning values?
Hi Irene. The key thing about HRV is that it varies quite a bit, so you can only compare readings made at the same times of day. This article illustrates the point quite well: https://www.myithlete.com/how-your-hrv-varies-throughout-the-day/
So I really wouldn’t worry about nighttime readings, unless you have a sleep condition like sleep apnea, and indeed focus on the waking reading in the standing position.
Hope this helps!
Simon.
Ah been using the ithlete for other a month now and my hrv has been superb most days with scores of 90s to 100s. This is puzzling as I am a combat athlete in the last 3 weeks training before a fight, so naturally my sympathetic system should be higher due to the amount of hard anaerobic sessions I’m am attending atm.
How are we accounting for the low resting hr in the 1st place?. Is this seated, standing or lying down?
As mine is mid 40s lying down slowly raising to mid High 50s when I stand.
Regardless I have a month’s data of lying readings which, i will now stick to the standing readings for a more accurate baseline.
Hi Joshua,
Medically speaking RHR would be measured laying down, so we’d suggest that to assess your base.
Thanks,
Laura