
Atrial Fibrillation (AF) and HRV
Heart rate variability (HRV) is all about analysing variation in the beat to beat intervals of the heart.We measure the rhythmic increase and decrease in heart rate as we breathe in and out. That’s called respiratory sinus arrhythmia (or RSA for short). It is a natural, healthy phenomenon, in fact the more variation the better!
But some heart rhythms are not healthy, and potentially dangerous. One of the most common heart rhythm disorders is called Atrial Fibrillation (A-Fib or AF). This is when the top chambers of the heart beat faster, and out of sync with the bottom chambers. It’s not life threatening, but AF reduces the heart’s output by about 30% and also churns up the blood, making it more likely to clot, potentially leading to stroke.
Although AF is most common in older people with conditions such as obesity, diabetes and heart disease, it’s also quite common in masters age endurance athletes, particularly those with a long training history. Champion Kayak surfer Oscar Chalupsky recently reported his experience with AF in this podcast.
The new research
Now a new study has come out sponsored by the US National Heart, Lung & Blood Institute. It looks at data from a large study where subjects were followed up for an average of 20 years, allowing them to identify factors such as HRV and resting heart rate which might predict the chances of contracting AF years later.
The researchers looked at the HRV and resting HR of 11,700 45-65 year olds from multiple ethnic backgrounds. They looked at how many people then developed AF during an average follow up period of 20 years. The study captured lots of lifestyle data such as smoking, alcohol use and the presence of existing medical conditions.
What did they find?
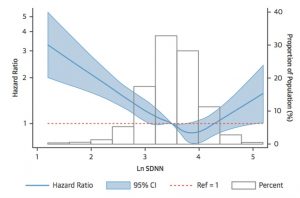
The first thing they found was that the likelihood (Hazard ratio) of contracting Atrial Fibrillation reduced with increasing HRV. This is not surprising, since as well as being a generally good thing for health, more HRV has also been shown in previous studies to be ‘cardio protective’ i.e. it protects the heart against potentially lethal arrhythmias.
What is a little more surprising is that there seems to be an optimum amount, above which the risk of AF seemed to start increasing again.
This is shown more graphically in what they found about resting heart rate (expressed as RR interval = 60000/HR):
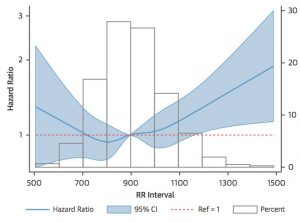
The optimum resting heart rate is therefore 60000/900 = 67 bpm, relatively high by athletes’ standards. A resting heart rate of 120 bpm makes you about 20% more likely to develop AF. But a resting HR of 40 bpm actually makes you nearly twice as likely to develop AF within the next two decades as someone with a resting HR of 67 bpm!
What does it mean?
I expected the main message of this study to be that higher HRV and lower resting HR (which usually go together) are always better, and this is true up to a point. The authors use this nice diagram to explain how this portion of the findings works, mostly for sedentary and less lifestyle conscious people:
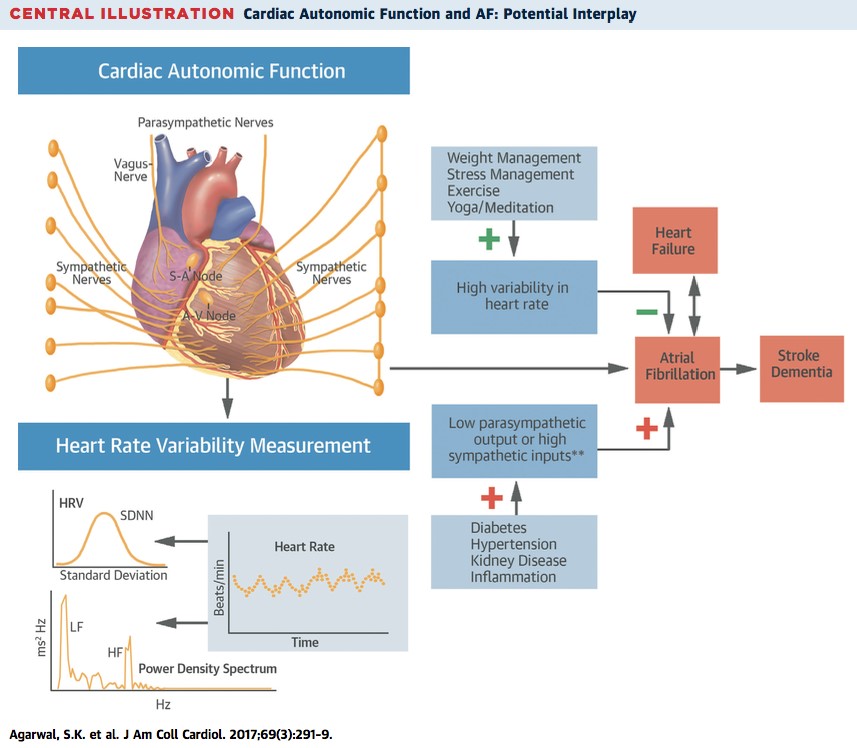
For the increased risk associated with low resting heart rates and high HRV, the mechanisms are more elusive. In the case of Masters athletes, years of training have caused extensive cardiac remodeling. Not only do the chambers of the heart become greatly enlarged, but the muscular walls include more scarring and fibrous tissue, which can interfere with the heart’s normal conduction system. This can lead to spontaneous contractions of the upper chambers (atria) during episodes of AF which are more likely to occur during periods of stress, either mental, physical or chemical, e.g. due to alcohol or caffeine.
Summary
AF affects the performance of the heart, especially amongst older, less healthy people. But it also affects a significant percentage of Masters athletes. A large study over a 20 year period shows an interesting correlation between Atrial Fibrillation (AF) and HRV. There are optimum values of HRV and resting heart rate, above and below which the chances of developing AF increase significantly.
Track your HRV & RHR with ithlete
If you suspect that you do get AF occasionally (or continuously), there is an app by a German company called Preventicus which is medically certified and which can perform a one minute test using the free version to tell you whether you are likely to have an irregular rhythm that needs investigating.
There are also help & information groups such as afa.org.uk (@AtrialFibUK) and anticoagulationeurope.org (@AntiCoagEurope).
As a 60-year-old semi-athlete that was diagnosed with atrial fibrillation in 2016 and just had a cardiac ablation in July 2022, I was wondering if there have been any studies regarding using HRV to assess the effectiveness of cardiac ablations? For instance, measure HRV before ablation and 3 months after ablation and track subjects for 5 years to assess recurrence of afib.
Hi Dave,
Apologies for the slow reply. I’ve been thinking about this but haven’t found any relevant research to help. Since AF is caused by extra conduction pathways in the right atrium, I don’t think that HRV would directly reflect any neurological changes following the ablation procedure. But since HRV reflects all kinds of stress on the body, it’s quite possible that HRV would increase afterwards due to the fact that you are just generally feeling better, less anxious.
Hope this helps, best wishes for remaining AF free, Simon.
Simon
I tried to take my hrv with your app today. After six tries I gave up & made coffee. I am one of the master athletes described in the AT article. I am 66, just retired back into northern BC. With the move came a new health region. I was set up for a complete medical. The EKG was flagged up & I was sent into town to wear a halter HRM overnight. I’m waiting to hear from the cardiologist. I’m in little doubt my issue will be the long term remodelling from high training loads. I did hear ‘enlarged atrium’. I did notice this morning that my HR was pretty wild, lows of 30, finally measured at my wrist as 59. Will iThlete be able to measure my hrv? Or do I need more sophisticated (& expensive) equipment?
Hi Les. Thanks for the comment, and sorry to hear about your EKG. It is indeed quite common for Masters athletes to have conditions like occasional atrial flutter and atrial fibrillation (AF).
It is not possible to measure your HRV whilst in this condition, irrespective of the price / complexity of equipment BUT the recommendation is equally clear – ie to avoid high intensity training whilst it is going on, so in a sense you don’t need the HRV measure. When you are not in AF (which is hopefully the majority of the time), you should be able to take your HRV without a problem, but please always follow your cardiologists’ advice regarding maximum exercise intensity & heart rates.
btw some old school thinking on risk factors such as caffeine for AF has recently been overturned: https://www.velopress.com/caffeine-heart-conditions-athletes/
Hope this helps,
Simon.
I am 65 and an age group triathlete – but only up to 3 hours if so duration. I had AF mid triathlon (in mid Russia!) two years ago. I finished the Tri by walking – unable to run – and ended up in Cardiac ITU. Echocardiogram etc. didn’t reveal any abnormal sizing and I’m not on any meds. I bought a 6 lead KardiaMobil ecg device and do an ecg after each training session. It has detected unsymptomatic AF 3 or 4 times in 2 years. The ecg it produces had the same pattern as the Doctors full 12 lead. I’d recommend buying one, £150. I continue to compete but do intense sessions less often (80:20) and ease off when my HR exceeds 170. I am waitlisted for ablation.
I had the ablation 6 months ago after getting AF a few times during slow bike rides and then just loafing around at home. AF has not repeated since ablation. Resting HR has risen from 60 before to 70 since ablation. Only do low intensity exercise at the moment, would love to get back to triathlon but I’m not optimistic. Shux.
That must be frustrating Cliff, but it’s always best to proceed with caution. All the best with it!
I am kind of confused about this. Using an oxymeter, I can see my oxygen level from my finger, and also the continually changing beats per minute. These change every part of a second and go from the fifties through the eighties for the most part. Are these different beats the HRV? I thought that this was bad and it indicated atrial fibrillation as well as it being an irregular pulse. I got this condition after a failed ablation for atrial flutter, when I was sent to the ER with a very high pulse and an irregular one. I had had this before during that high stress month, but it always went back to normal after the episode. Once they did the ablation, my heart beat on the oxymeter and on the blood pressure machine showed this variability as a shaky heart symbol on the blood pressure machine and going through different rates in split seconds on the oxymeter. Is the only way to determine atrial fibrillation to see it on an EKG? I have my next appt in a couple of months, when I will have an Ultrasound to see how my heart is doing overall. And I am on a low dose beta blocker to keep the adrenaline lower due mostly to the stress of allergies. Just curious about your take on this variability issue. Today is the first time I came across it .
hi Irene,
HRV describes the changes in timing from one beat to the next, especially as you breathe in & out: https://www.myithlete.com/what-is-hrv/
Nearly all HRMs and pulse oximeters smooth out these variations & report the average HR over 5-7 beats, so they don’t report the kind of HRV we are looking at for exercise recovery.
If your pulse rate is varying a lot whilst you remain still, that is likely related to your condition, and not to what’s called parasympathetic or vagal HRV.
A number of endurance athletes do get occasional AF, which they can often feel in their chest. The ithlete app can detect irregular beats & won’t let you take an HRV test whilst it is going on, but you can use HRV to measure recovery whilst you are in Normal Sinus Rhythm (NSR). Hope this helps – there are lots of good articles on the web from certified medics describing AF & other arrhythmias.
I bought an apple watch on July 2020, came with an EGC app. Shows Atrial fibrillation to me, I was annoyed, then I told to my friends to wear it, all of them showed “sinus rhythm” but for me AF, so I went to the doctor who performed an real ECG, which confirmed the presence of AF.
Regards
Hi Luis
Good that you have the AF diagnosed now. Do you need treatment, or can it be managed by lifestyle changes?
best wishes,
Simon
Thanks for your blog and many very valuable posts.
On this instance, as you sum up the work pretty neatly, it looks as if AFib occurs when the heart reaches its function boundaries. in other words the hazard ratio increases outside the HRV distirbution bulk!
What’s your opinion?
Cheers
Thanks for the comment Willy (nice Anglicisation of your name btw!). Yes, I think it’s primarily a heart size related phenomenon. Endurance exercise increases heart size & circulatory function up to a point, then further enlargement causes scarring of the top chambers (atria), increasing the chances of electrical disturbances inc AF. On the other hand, a smaller heart is associated with lack of exercise and some CV diseases, and again the chances of AF increase. So there is a sweet spot of minimum AF for resting heart rates of 55-60 bpm.
I am a 64 year old male. I’ve been active all my life. I was recently diagnosed with afib. I have an Apple Watch and noticed that in afib my HRV is between 190 and 245ms. When not in afib my HRV is between 45 and 65ms. I have a low resting pulse of 45. Are the pulse and HRV numbers concerning?
Hi Dave
Thanks for the comment. It’s not unusual for Masters athletes to have AF – often due to scarring of heart tissue from years of training, which enlarges the chambers of your heart – hence the low 45 bpm resting pulse.
When you get the high reading – it’s not actually LF/ HF HRV you are measuring but artifactual beats that have unusual timing due to the atrial firing.
When ithlete does an HRV calculation, it tries to exclude these artifactual beats to give a (more) representative measure. Please note also that the Apple watch measures a somewhat crude all inclusive HRV measure called SDNN, rather than the RMSSD used by ithlete to indicate stress & recovery. Hope this helps! Simon.
I have Afib which developed after two aortic valve replacements 12 years ago. My aortic valve was destroyed when I contracted endocarditis. I was born with a bi-leaflet aortic heart valve. The second mechanical valve was a redo when the 1st surgery failed. I have Atrio Flutter. They made two attempts to cardiovert without success. My cardiologist says I’m not a candiadte for ablation.
I am a strength trainer and state champion bodybuilder. I ran mile intervals for over 20 years at a 6:30 minute pace at 190lbs; my cardiac fitness declined duringa. 4 month hospital stay. Given I am 65, I opted to stick to hiking and biking for cardio. I rebuilt my muscle size and strength within 4 months of hospital discharge.
I wear an Appl Watch and noticed my HRV is consistently above 200, occasionally spiking to 300. The lowest values are above 125. My resting heart rate is 40-45 when I awake each morning. Daytime HR between 55-70. Hiking HR 100-150 on uphill.
Is such a high HRV normal or is this cause for concern? As I said earlier, I hav Eno loss of energy, except when I attempt to workout as intense as before I contracted endocarditis and had surgery. I believe I could return to the intensity I once had, but believe fitness after 60 isn’t gauged on speed or intensity, but consistency and feedback from vital signs. Since I don’t intend to compete in any masters competition, what I’m doing should be satisfactory for living a energetic and quality life. Should I be concerned about my HRV?
Thanks for any advice or information.
David.
Hello David. Thanks for the description – sounds as if you are a lifelong training enthusiast, and want to keep going as much as possible into later life. Me too!
The reason your HRV is reading high is very likely due to the atrial flutter / fibrillation, which causes the ventricles to beat irregularly, though overall at a sensible rate (as evidenced by your resting, and exercise HR values). If this AF is continuous then there’s really nothing to be gained from HRV measurements, as these rely on nervous system input to the right atrium during normal sinus rhythm.
So I think the resting & exercise HR values are the useful metrics for you. I’m not a medic, and would recommend that you see your cardiologist regularly to discuss your exercise program, and to ensure you are taking the right anticoagulants, if those are needed.
Hope this is helpful, all the best,
Simon.
Simon-
Thanks for the salient advice.
What do you think about the heart math technique? As I understand, positive and negative emotions can improve the HF/LF ratio and higher HRV readings are indicative of good heart health? I also read that higher ratios improve hormones and reduce cortisol. I supplement with DHEA and am a very positive person. I am 66 but as fit and strong as men 20 years younger.
Your advice that reading HRV via Applewatch may not be as valuable feedback as resting and maximal heart rate seems logical to me.
After aortic valve replacement 12 years ago, I have relied on hiking, biking, walking and lower intensity aerobic exercise to stay heart healthy. I have consistently stayed with strength training since my teen years only pausing during my 4 month hospital/cardiac rehab in 2008.
I’ve decided I want to increase the intensity of my aerobics by running, as I miss the “runners high” I exeperienced when doing HIIT. I find limitations related to respiratory function. My cardiologist is scheduling a pulmonary function test to help discover if I have limitations related to breathing. I had two tracheal dilations within 2 years after HVR and my trachea may have stenosed such that my respiratory function can’t keep up with my heart demands.
I do recognize that my exercise intensity over 20-30 years may have contributed to the onset of my Afib and I certainly don’t want to return to the high intensity training, if it may be detrimental to my health.
As you may have noticed, I am a person who is trying to maximize my human potential, both mentally and physically. If experimenting on myself helps me become an successful example of what is possible, it may help others.
Thanks for your advice and expertise in this area.
David
Hi thanks for this article. I am a 43 yr old Contortionist who has never considered my self elite an athlete. But I train 16 hrs a week . I think I have always had a arrythmia but recently with stress everything (heart) got bad. My heart was racing and pounding hard and I was light headed and dizzy . It was fluttering a lot. Anyhow I went to the acupuncturist and she mostly fixed me up. But I thought I should measure my vitals until I can get health insurance and a doctor. I got a morepro watch that measure BP and does an ECG…with that is does HRV. It always says that my HRV is normal but I don’t know what values are normal. Or how account this watch is. I figure it isn’t great. It is supposed to measure just HRV but it doesn’t. It does do heart rate and oxygen. My question is what are normal values especially if you are an endurance athlete? Also my ecg has not once been normal. I do plan on seeing a doc. I Just wanted to bring in collected data.
I do know my RHR is pretty high. (80-90’s but occasionally drops to 70 depending on my relaxation technique) My peak HR ( when I am working the hardest hits about 140) and I do know I don’t know HRV and what I should look for ? Also BP seems high . The watch can not measure ecg when I am working out I think which means I am not getting a clear readinf of HRV then. It just goes crazy. So do I just measure in the morning?
Any thoughts…also I would like to invest in another device if it is more accurate and will help. Which might I get for needs?
Hi there – glad you found the article interesting, and apologies for the slow reply – we’ve been busy on a few different projects, mostly Covid related.
We can’t give medical advice on this blog, but I would highly recommend getting your arrhythmia properly diagnosed by a cardiologist, and not spend time gathering data first. Data I would collect in this situation is the timing & duration of the arrhythmic events, plus contextual data which will aid interpretation, such as your daily diet, stress management & sleep. Your morning resting heart rate may also be useful, but I would leave the HRV as it cannot be measured accurately whilst the arrhythmia is going on.
Hope this helps, good luck with having the condition identified & treated.
That helps a lot as I am finding my HRV is all over the place . Lows in the single digits and a high of 80’s. Thanks. I won’t worry about HRV for now.
Kia ora.. thank you for all of the above.. quick question.. . Could it be possible that the HRV reading went unusually high if there was AF going on ? I’VE had AF in the past and the other day my HRV went unusually high…and I’m wondering could this be related ?
Hi. I have been using your app for around 4 months. Some days I get a fair number of PAC’s. I note that on these days two things happen. The first is that I get a “measurement stopped early” message. Then, if I get a successful reading, it is quite high.
On another app, where I can see my recording live, PAC’s and compensatory pause results in a spurious increase in HRV. The “other” app identifies some, but not all of the ectopic beats and corrects those it identifies.
I predict that the apps are misinterpreting the electrical data.
Of course this has implications for training as the results impact baseline.
Can you please comment on this.
Hi Steve,
Thanks for the feedback. Indeed it is very challenging to screen for all premature atrial contractions and other arrhythmias automatically. We use techniques tested in the literature to identify these and stop the measurement early, but for medical screening, the ECG trace would be examined by a cardiac electrophysiologist and all abnormal beats would be marked. The problem with letting the PACs / PVCs through is that they will exaggerate the HRV reading. The apps are not misinterpreting the electrical data, but rather, the R-R intervals of the heart are not in the normal sinus rhythm assumed in the calculation of HRV. Whilst we would not recommend anyone uses ithlete with continuous arrhythmia, if you are able to feel the PACs / PVCs I would suggest to stop the measurement (if the app does not do this for you). Hope this helps.