
Who, What and Why
Back in 2009 we had a report from one of the original ithlete beta testers that during an ultra endurance event he got an unusually high waking HRV, despite feeling totally fatigued. We have been intrigued ever since by the notion that the balance between sympathetic and parasympathetic can shift too far towards the latter, which is of course the opposite direction to what most people expect when too high stress levels have taken their toll.
Most of the research has focused on the more commonly occurring reduction in heart rate variability (HRV) with increasing training loads and stress, and good quality studies on parasympathetic overreaching have been lacking, but recently, two studies from sports science infographic supremo Yann Le Meur at the French National Institute for Sport shed more light on how & when this form of overreaching occurs.
What Did They Do?
In the first study, 24 well trained triathletes (who trained at least 6 times per week) took part in a 7 week study and were separated into two groups. Eight of them acted as a control, and performed their usual training, whilst the other 16 volunteered to have their usual training load increased by 40% for a period of 3 weeks in the middle of the study period. Both the session durations and the number of high intensity repetitions were increased to deliberately induce overreaching. Training load was monitored using time in each of 3 zones (Lucia TRIMP), and the zone thresholds were also re-measured during the study in case they had shifted.
HRV was measured every morning in both lying and standing positions for the 3 intensified weeks and the taper week either side. RMSSD and resting HR as well as HF & LF frequency domain parameters were calculated. Subjective tiredness was also recorded once per week using a 0-100 fatigue scale. A weekly maximal running test on the track was used to verify overreaching i.e. that performance was significantly worse than that of the control group in spite of continued training.
In the second study, the researchers decided to use a parameter called heart rate recovery (HRR), which is measured at the end of a standardised exercise, and is often considered to reflect progress in overall fitness. Basically, if an athlete’s heart rate recovers more quickly after stopping exercise, they are considered to be fitter than they were previously. The rate at which HR decreases after exercise depends on the rate of sympathetic withdrawal, and parasympathetic reactivation, so this additional measure of ANS balance could give additional insight as to the mechanisms behind reduced performance whilst in an overreached state. They also studied well-trained male triathletes before, during and after a 3-week overload period. HRR and blood hormone levels were measured after a maximal cycling test performed before and after the 3-week overload period.
What Did They Find?
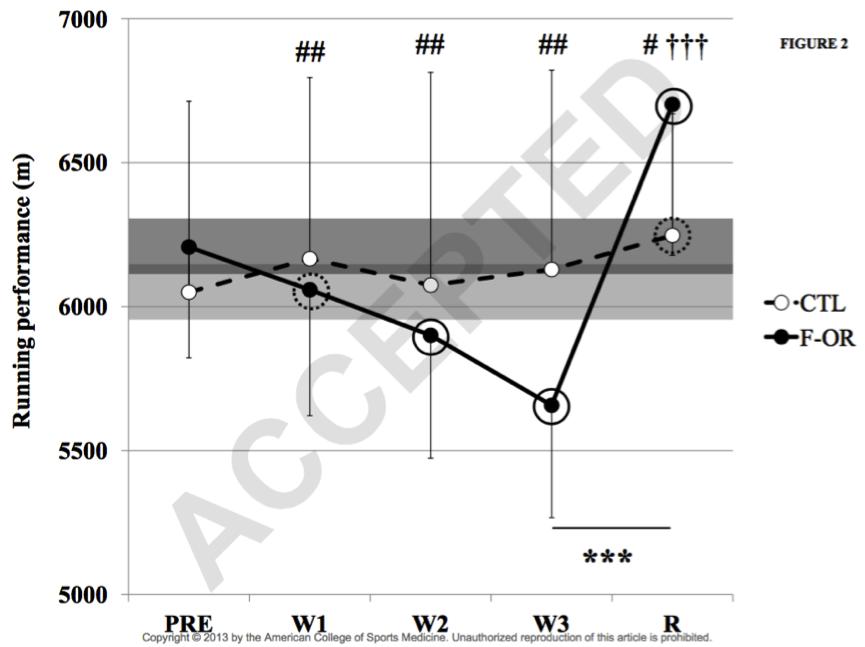
They found that 15 of the 16 intensified training group (F-OR in the figure) showed decreased performance after the overload period, so the overreaching had been successful in all but one case (whose data was then excluded from further analysis). Performance then rebounded after the rest week, proving that the overreaching was functional, whereas recovery from non-functional overreaching takes several weeks or even months.
The heart rate measures demonstrated consistent patterns, but with varying degrees of significance:
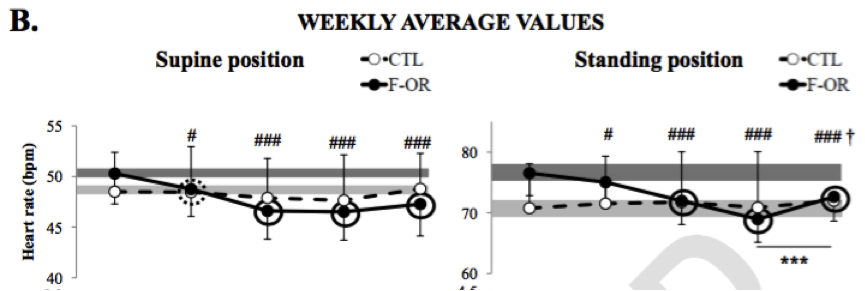
- Resting heart rate (RHR) decreased during the overload period.
- The decrease was more progressive and significant in the standing rather than lying position
- Significance was greater using weekly moving averages than single day values
- RHR increased back towards, but did not reach pre-overload levels after the rest week
- Time domain HRV (LnRMSSD) increased during the overload period
- Single day isolated measures only achieved significance after the third week, irrespective of body position
- Weekly averaged values reached significance after the first week
- The standing position appeared to give the greatest sensitivity, especially in respect of the decrease during the post-overload rest week


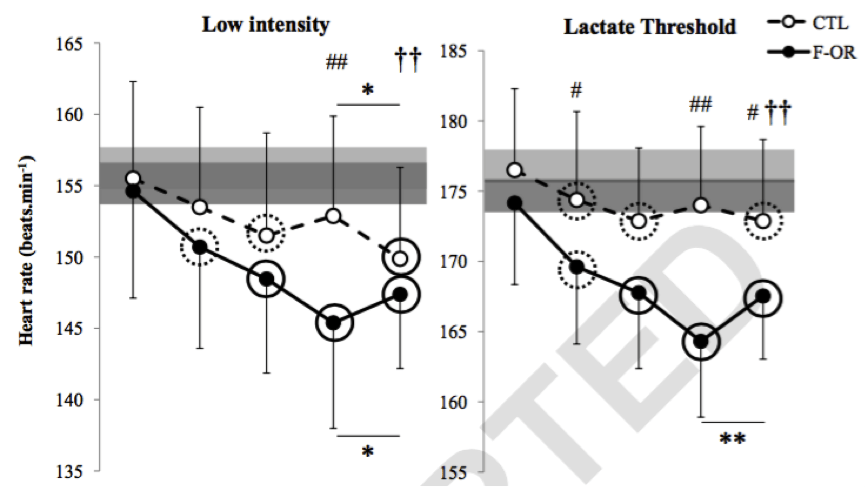
What was also notable from this study was the heart rates at low intensity and threshold, which also decreased very significantly during the overload period.
In the second study, the researchers found that many (though not all) of the athletes in the overload group met the criteria for overreaching (f-OR) after the overload period, and that their heart rate recovery increased very significantly, reducing again during the subsequent rest week. The remainder of the overload group (AF) also showed a likely increase in HRR, but as the diagram shows this was less significant:
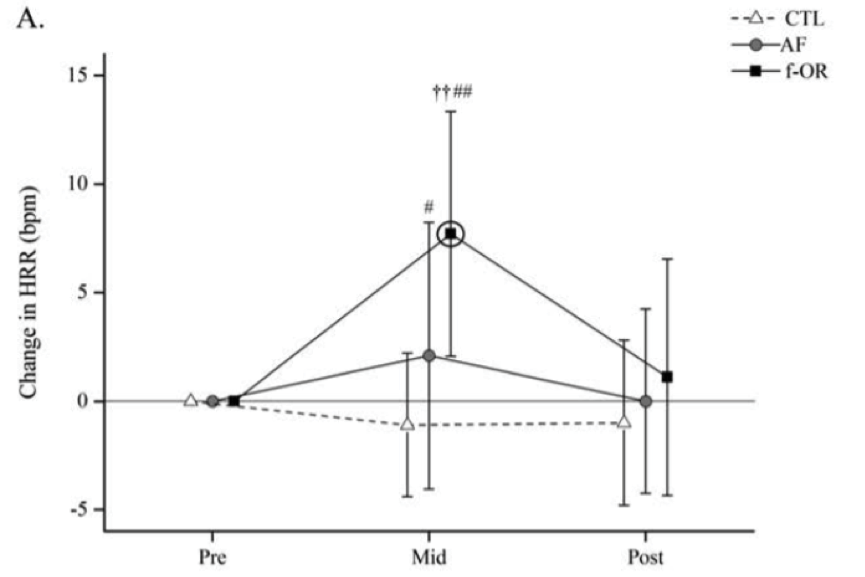
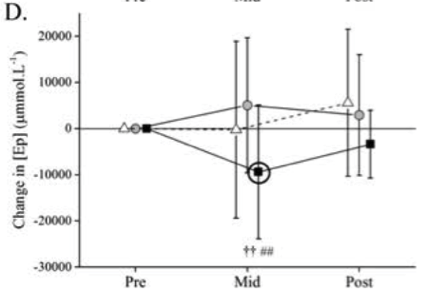
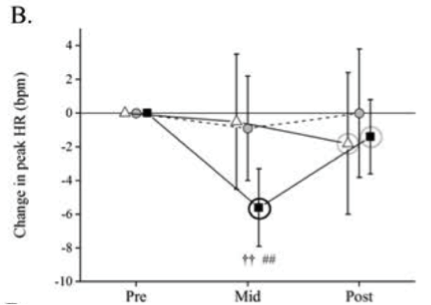
This increase in HRR was therefore associated with reduced performance, rather than improved performance, its more usual interpretation. What’s also very interesting is the decrease in peak exercise heart rate (B.) and epinephrine (adrenaline, D.) concentration in the overreached group:
What does it mean?
The first study clearly demonstrated trends in resting HR and HRV that are opposite to those often expected and experienced by recreational athletes. The study group were relatively serious athletes, training 10-12hr per week regularly, and achieving times of 2:00 to 2:20 in Olympic distance events. Training time was increased to almost 17 hours per week during the overload period, which is needless to say a big increase on the load and well beyond the more usual 10% per week increase, which most athletes can tolerate.The second study also clearly showed a relative parasympathetic dominance using the HRR measure. This study also measured blood adrenaline levels significantly reduced in the overreached state.
Despite the very clear results, the mechanisms behind these alterations are not fully understood yet, and the authors suggest can be caused by a combination of 3 effects:
- A decrease in central command – ie less internal stimulation during intensive exercise
- Reduced chemoreflex activity (with lower accumulation of post exercise metabolic products)
- Potential changes in autonomic control
Practical suggestions for HRV and resting HR measurement interpretation
Rather than always interpreting HRV rises as a good thing, we recommend putting HRV rises into context as follows:
- In a fast-rising HRV trend situation, look at resting HR as well. If it is decreasing fast, you may be heading towards this form of overreaching. The ithlete mobile app includes colour coded indicators for these trends, but the ithlete Pro Training Guide allows them to be followed more precisely, and using a standardized scale of standard deviation units, which are comparable between individuals and over time:
- If using heart rate recovery (HRR) as a post exercise measure, look out again for fast rising trends over a few days or a week. Aerobic fitness does not increase that quickly, but takes several weeks
- Record subjective mood and fatigue indications and be honest with yourself – if you feel tired and a little demotivated, record it that way. We wrote a full post about tracking your subjectives here.
- Record Training Load and calculate a weekly average. If this is increasing more than 10% per week, then overreaching is a distinct possibility.
By Simon Wegerif
References
Evidence of Parasympathetic Hyperactivity in Functionally Overreached Athletes Yann Le Meur, Aurélien Pichon, Karine Schaal, Laurent Schmitt, Julien Louis, Jacques Gueneron, Pierre Paul Vidal, and Christophe Hausswirth. Medicine and Science in Sports and Exercise. November 2013
The development of functional overreaching is associated with a faster heart rate recovery in endurance athletesAnaël Aubry, Christophe Hausswirth, Julien Louis, Aaron J Coutts, Martin Buchheit & Yann Le Meur PLoS ONE (Impact Factor: 3.23). 09/2015
Very interesting article but I think I will have to read it a couple of more times to fully understand it. I have always wondered about a high HRV coming up red on my ithlete Pro.
What I have found in my experience is that the high HRV rebound reflects an immune over compensation via activation of a side of the immune system that deals with anti-inflammatory effect (i.e. IL-10 etc…). Often this is also accompanied by a very different value from supine to standing compared to normal. Yet, according to my research the exact mechanisms of this process are not fully understood. As mention in this article if the HRV is quite high as a rebound effect in response to high load (both timely and intensity) I normally suggest to keep the recovery at least until it has stabilised back in average ranges.
Thanks for the observations Alex. As Alan Couzens observed on Twitter relating also to this research – ‘Just like 3 bears – not too high, not too low. Best training comes when HRV is just right.’
…and they all lived happily ever after with the ithlete Pro Training Guide!
HRV is very personal, and can be very high as in my case when HR is very low, using a forced breathing protocol you can at least make the measurement reliable. Standing can offer a more reliable position compared to seating in that case, but upon establishing your own baseline it allows anyway to look if you are recovered or not from the last training.
Highly interesting, I’m an amateur cyclist just having completed a full months cycling in Mallorca. I was noticing this a lot today, difficulty in achieving threshold heart rate, some 15-20 bpm off and seeing my heart rate fall much lower than i would normally when well rested. The body was certainly not willing today!
Thanks for the feedback, Rob. Although a lot of people have noticed this effect, it’s still not fully explained by science. Whether it’s due to a fall in adrenaline production, or a protective downgrade in sensitivity to adrenal hormones, or something else, no-one seems quite sure. I’ve been there, and can also testify that ‘the body is not willing’! Hope you enjoyed Mallorca – I just signed up for the 312 again next year. Simon.
Simon THANK YOU. Not sure why I only saw this now, but your articles are always extremely useful and interesting. The body is indeed a complex mechanism. I think it also helps tremendously that you are not just a scientist but a practising athlete who can speak from experience.
Thank you Sonja for your ongoing support! I do continue to find the complexities of the body fascinating, and often ponder how the various mechanisms evolved to be like they are today.
We have quite a few articles in the bank and plan to organise them better for users and anyone interested in HRV to access.
Any ideas on how I might reduce my HRV, which was as high as 105 three weeks ago and has been hovering at 100 for most of the time since.
Hi Sonja. A few questions to try & identify what might be happening: Is this value unusual for you? What is your normal range, and how does the accompanying resting HR compare with your normal values? Are you performing well and really fit at the moment, or are you chronically tired?
Hope we can get to the bottom of it for you!
Simon
Hi Simon!
I’m super intrigued with this.
I have an unusually high HRV (averaging 130-150ms with a high of 200. I wear the Oura ring, so it only tracks while I’m sleeping).
– I get terrible sleep (I average about 4-5 hours/night due to work), but tend to fall asleep very fast.
– Most days, I have no problem and am not tired.
– My HR stays about the same, between 40-50bpm.
– I workout about 3-5 times per week. A mix of endurance, strength, and interval style.
I’m a bit concerned about how high it is, because it often crosses 200ms. I have data from my Oura ring, so I wanted to get to the bottom of it and haven’t found ANYBODY with that high of an HRV. any thoughts?
Hi Adam. Thanks for the comment. Yes, as a raw rMSSD measure, that is high. For a number of reasons, we use a (patented) log scale in ithlete where very fit endurance athletes score ~100.
Your number equates to 106 on the ithlete scale, which is high, but not the highest we have ever seen (that was 116 from an Australian football player).
Whether it’s the right number for you depends on your genes, training history, need for sleep & current state. It also depends on how good the Oura ring is at detecting artifacts, as these can easily distort the value (nearly always increases it).
I’m not a big fan of sleeping measurements lying down, as these can suffer from what’s called parasympathetic saturation.
In our view, you’re better off taking a short paced breathing reading in the sitting or preferably standing position every morning.
Best, Simon.
Hi there. Can you elaborate on parasympathetic saturation?
Hi Liz,
Parasympathetic saturation refers to a phenomenon where the vagal ‘brakes’ to the heart are on full – ie the heart rate can’t go any lower. This tends to happen in endurance athletes when lying down. Since HRV measures parasympathetic (vagal) activity, this can mean that you don’t see any change in the HRV number from one day to the next. That’s why we recommend performing HRV measures in the seated or (better) standing position, since the extra work required from the heart to pump blood uphill means the brakes have to come off, and you will see meaningful day to day variation in HRV.
Hope that helps!
I started tracking my HRV with WHOOP band. My high values are 139-180, with few lows of 25-80 ( and 25 was when I felt sick ). I also checked my Apple watch HRV data and it seems to be spiking above 140 often. I am 33y old female and do about 1 hr of weight lifting 5-6 times a week. I am a bit worried since it looks like a good hrv for my age should be around 60. My Resting heart rate stays around 45-50.
Hi Victoria,
We really can’t comment on numbers produced by whoop. I don’t know what number system they are using or if they are accurate, and therefore if you need to be concerned. I would contact their support.
Best wishes, Laura
Hello Laura,
I have since been using Oura ring as well. And my average number is around 150 HRV and 48 Hr. The highest I get is in 190 range. Still training 5 times per week.
Hello Victoria. I am 66y. Began using Kubios Windows at 60. Using Kubios app today. Tried Whoop. 150-200 HRV (RMSSD) is just where I was and where I am. It will eventually go down to <90 immediately after a long workout. The max Whoop reported is 210. EliteHRV and HRV4Training will compare with their user database. My values would already way too high for a 25y young people.
Hi Adam,
It’s been a few years since you made this comment on the ithlete site:
– I get terrible sleep (I average about 4-5 hours/night due to work), but tend to fall asleep very fast.
– Most days, I have no problem and am not tired.
You say you’re not tired most days. Do any of your relatives function well on little sleep? Is it possible that you have the short sleep gene?
Hi, I have an ithlete and a FrontierX and am confused by the scale used by ithlete. I understand the scale is patented but can you give me any idea of how it compares to millisecond data? E.g a score of 70-80 on ithlete would be approximately what using milliseconds? I ask because the results from ithlete and Frontier X appear vastly different and I’d like to figure out which is more accurate or if in fact they match just on different measurement scales.
Hi Amber. Sure, the ithlete scale (and why we chose it) is explained here: https://www.myithlete.com/hrv-scoring-system/ To answer your question specifically, 70 on ithlete is equivalent to 33ms and 80 to 55ms.
We hope that helps, and that you enjoy using ithlete (ithlete was the first HRV app / wearable to be independently validated, so it should be accurate!).
I am 79y, do cardio and muscle exercises, also brisk walking 4 times a week. Have used an Apple Watch for 3 weeks. HR resting average 60bpm. Walking 109. BUT HRV ranges between 145 and 210, average 180ms. Surely this HRV is not normal especially for my age.
Hi Lesley,
Thank you for reaching out. We are unable to comment on HRV data from another device/system. If you would like to try ithlete we offer a free trial here and would be happy to assist with any queries on your data from there.
Best, Laura
Sleep number bed data shows HRV average of 196. I am 66 years old and average about 20 miles a day on my bicycle. Very active. Can this be an accurate reading? Most HRV scales I see end at 100.
Hi Ken,
Unfortunately, HRV scales do vary between devices, even when the underlaying measure (often RMSSD) is the same. The ithlete scale, created in 2009, uses 20 * LN(RMSSD) which we think makes sense because fit people do have numbers up towards 100 (even though this is not a hard stop), and 1 point on the scale is about 5%, which is the smallest worthwhile change in daily use for most people. I would expect your ithlete HRV to be in the 70-85 range for a fit 66 yr old.
The East Germans did a lot of research on overtraining, and their “Principles of Sports Training” manual described two types: excited overtraining and depressed overtraining, which probably correspond to sympathetic and parasympathetic overactivity. For “depressed overtraining”, as I recall, they suggest using alternating hot and cold showers, taking a break by the sea (for excited, it was a break in pine woodlands).
The book is well worth reading (as much for ideology behind it as the meticulous sports research…though their research into use of anabolic steroids was conducted in secrecy.
https://www.amazon.co.uk/Principles-Sports-Training-Dietrich-Harre/dp/0989619818
Simon, I love this article and your other article “9 Common Misconceptions About Measuring Heart Rate Variability.” In that article, you wrote “the body gets tired of producing adrenaline and becomes less sensitive to it, possibly as a mode of self-protection from highly driven type-A personalities” – and this describes me to a “T”! Recently, I’ve noticed that my high HRV and low HR seems to correspond to feelings of fatigue – but early in July, high HRV and low HR felt “healthy.” Is there any way I can identify the difference between “good/healthy” HRV and “bad/fatigue” HRV by looking at different data?
Hi Diana,
Thanks for the feedback and glad you like the article! To be honest it is quite difficult to distinguish between “good/healthy” HRV and “bad/fatigue” HRV except by using context ie whether this combination appears after a period of intensified training, or a period of rest. Hopefully the wellness metrics and acute:chronic training load ratio can help you distinguish between them.